So, autism (further also ASD - autistic spectrum disorder) is a tough nut to crack - I’d even call it the king of neurodiversity disorders. It’s:
polygenic
extremely diverse in regard to manifested traits and their power
comorbid with a lot of stuff
can both enhance chances for life success, or be a serious disability (75-90% of autistic individuals are unemployed in different countries, one of the highest rates)
P.S. It’s important to disclose the diagnosis to potential employer - it increases the employment odds by 200%
In an ocean of facts, one shouldn’t drown as odds ratio to do so if you have autism is 160x… But first I’ll drop the facts, and then try connecting them into graph-like pathways.
Influencing factors
Genes and comorbidity
First of all, let’s uncover the ‘polygenic’ and ‘comorbid’ claims.
A recent study had uncovered genetic variants that influence the development of several disorders (eight to be accurate (8.0 to be even more accurate): autism, ADHD, schizophrenia, bipolar disorder, major depressive disorder, Tourette syndrome, obsessive-compulsive disorder, and anorexia. These variants are called pleiotropic - ‘affecting many’, i.e. a gene affects the development of several disorders.
Plus previous study identified 109 pleiotropic variants and classified them by disorder pairs, of them the most prevalent:

So, it’s no surprise adding to comorbidity of ADHD (50-70%), and depression (up to 50%, but likely more as not all depressed autistics are diagnosed), psychosis is more prevalent in individuals with autism:

Wiki holds a nice Euler diagram for more genetic overlaps:

Even if we just take the first five, all seem pretty low-level (we’re talking ion channel/synaptic
CACNA1A encodes the alpha-1A subunit of P/Q-type voltage-gated calcium channels, critical for neurotransmitter release, neuronal signaling, and synaptic plasticity;
GRIN2A encodes a subunit of NMDA receptors involved in synaptic signaling, learning, and memory;
KCNQ2 encodes a potassium channel subunit that regulates neuronal excitability and action potential firing;
SCN1A encodes the NaV1.1 sodium channel subunit essential for neural signaling and neurotransmitter release (causes Dravet syndrome, epi-aut-schizo disorder;
the whole fun nine yards!);SYNGAP1 encodes SynGAP protein, a regulator of synaptic plasticity and brain development, critical for cognition and proper synapse function. Defects cause autistic-like behaviour.

Brain
First, cortical thickness - mightly frontal cortex for autists is here, along with up to 17% lower whole-brain synaptic density (particularly pronounced differences in regions known to be important for social and cognitive functions, such as the parietal cortex):

Also, the whole brain is hyperconnected in accord with MYT1L and pruning theory:

Now a bit deeper, onwards to social reward and reward connectivity…
Oxytocin, more brain and female autism
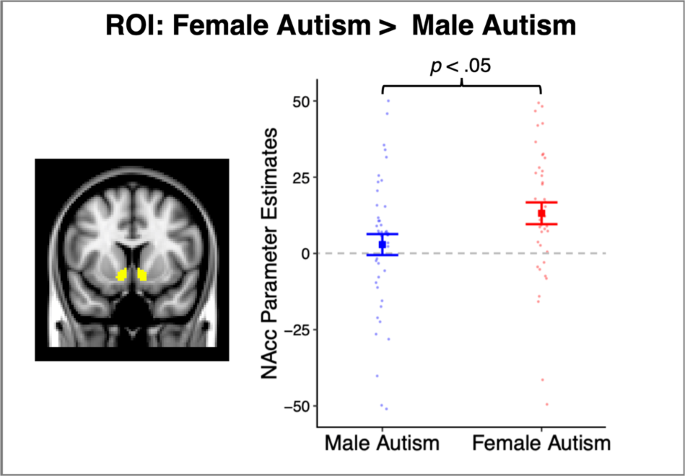
A fun study had explored oxytocin receptor ‘risk alleles’ and autistic phenotyping in males and females, with/without ASD (Pplxty):
for males, ⬆️ OXTR risk alleles:
⬇️ within-network connectivity
⬇️ nucleus accumbens ⇔ prefrontal cortex connectivity
whereas for ASD/NT females it was more alike to NT males, ⬆️ OXTR risk:
⬆️ nucleus accumbens ⇔ prefrontal cortex connectivity (possibly as a compensatory mechanism)
stronger nAcc ⇔ PFC and reward connectivity leads to higher social functioning scores
⬆️ NAcc ⇔ subcortical regions related to motor learning and sensory processing → ⬆️ scores for restricted interests and repetitive behaviours
Another older study confirms that decreased mesolimbic pathway density is causal to social deficits experienced by autistic ladies and gents:

It is said to partly confirm the social motivation theory of autism, where social interactions are less rewarding, leading to a vicious cycle (it could also partly explain the ‘cut the small talk/nonsense’ attitude expressed a lot in ASD → why engage in non-rewarding stuff wasting my time if we could just exchange the information and be done?)
Another new paper only confirmed this (higher autistic traits → lower social motivation) connection for females, though:

Yet autistic girls have expressed increased sensitivity for social rewards compared to boys:
Bear with me for a minute - so girls may still be less apt socially but are rewarded ~normally. Sounds like a difficulty diagnosing and a whole world of pain for them, isn’t it? Also, normal social connectivity despite OXTR deficiencies may partly be confirming the female protective model.
Interestingly, behavioral research suggests that high functioning females with ASD show greater social motivation compared to their male counterparts59,60,61, a finding which has been attributed to the ability of females with higher IQ to mask their social-communicative deficits60,62
There’s a great lecture by Sarah Hendrickx that further studies the sex differences in autistic phenotypes, summarized by the great
| Feature | Autistic Females | Autistic Males |
| Early Development | Often early speech and vocabulary; may be seen as shy or neurotic; may have tics; tomboyish tendencies. | May have speech delays; more likely to be diagnosed earlier (average age 5). |
| Social Interaction | Mimicry and camouflaging of social behaviors; may focus on social learning; intense desire for a single, exclusive friend; may be mothered by other children; better at socializing when young, but may struggle in teenage years as social dynamics become more complex. | Often prefer to be alone; may be less interested in social interaction; social skills may improve in teenage years relative to changes in females social world. |
| Interests | Intense interests often focused on people, animals, celebrities, or fictional worlds; may be seen as "little psychologists"; adult interests may include crafts, psychology, or true crime. | Traditionally, interests focused on objects (trains, dinosaurs, etc.); may be seen as "little professors"; more likely to be interested in numbers. |
| Behavior | May be seen as "clingy"; more likely to internalize distress (shutdowns more common than meltdowns); may be perfectionistic and helpful in structured settings. | May be seen as "loners"; more likely to externalize distress (meltdowns); may be more rigid in routines. |
| Cognitive Style | Strong verbal skills may mask underlying social and communication difficulties; may be organized and detail-oriented; may struggle with abstract social concepts; may create elaborate fantasy worlds. | May excel in areas requiring systemization and logic; may struggle with social nuances and non-literal language. |
| Teenage Years | Puberty and social pressures can be particularly challenging; may struggle with social rules and expectations; may be vulnerable to exploitation; self-harm and mental health issues are common. | May experience fewer social challenges than females during adolescence; may have fewer life events. |
| Adult Life | May have multiple jobs, relationships, and life crises; may seek diagnosis later in life (often in 40s); may be in relationships with other autistic individuals; may have a strong online presence in autistic communities. | May have fewer jobs and relationships; may be more likely to live at home longer. |
| Sensory Issues | May have sensory sensitivities to clothing, textures, sounds, etc.; may be more prone to stress-related physical conditions (e.g., migraines, fibromyalgia). | May have sensory sensitivities, but these may be less pronounced or less outwardly visible. |
| Mental Health | Higher rates of anxiety, depression, eating disorders, and suicidal ideation compared to autistic males. | May experience mental health issues, but potentially at lower rates than autistic females. |
| Diagnosis | Often diagnosed later than males (average age 8); may be misdiagnosed with psychiatric disorders; more likely to be missed in diagnostic assessments like the ADOS. | More likely to be diagnosed based on traditional criteria; more likely to receive a diagnosis based on observable behaviors. |
| Gender Identity & Sexual Orientation | Higher rates of identifying as non-binary, gender fluid, or having non-heterosexual orientations. | May have more traditional gender identities and sexual orientations, but variations still occur. |
Basically, we can roughly conclude that:
females with ASD may or may not exhibit social deficits on male level (likely it depends on a plethora of factors, not just OXTR and connectivity)
but still, they seem to have normally functioning social reward circuits
but definitely higher repetitive behaviour, learning alterations and restricted interests
all this stands to reason that females need to be a lot more autistic than males to get properly diagnosed, and often have to learn to mask properly on the go. Despite that, some studies tell that ~90% of ASD females had been victims of sexual assault - so much likely when you appear ‘normal’, don’t have healthy boundaries and don’t (yet) know the dangers. Adding to that - masking is often recognized as flirting

females have more desire to be socially acceptable, leading to more masking, leading to even more difficulties with diagnosis!
There’s a strong need for separate diagnostic scales, IMO. Some started to cater for that with e.g. checklists.

This may explain synaesthesia, sensory and word associations but difficulties with some complex domains requiring high density (vicious cycle of low density/low reward → no incentive to improve and increase density): social functioning, motor skills, diverse interests (requiring high intra-cluster density).
Inflammation and kynurenine, again
Along with kynurenine pathway:
ASD patients reported significantly lower TRP levels than BAP and CTL groups. Moreover, significantly lower levels of KYNA were reported in both ASD and BAP groups than in CTLs.
Reminiscing that kynurenic acid is an all-around anti-excitability and anti-inflammatory compound, we could hypothesize that inflammation can also be increased in autistic individuals (because kynurenic idea isn’t always confirmed by the research). Altered KYN/TRP (competing kynurenine - tryptophan pathways) and subsequent hyperserotonemia (serotonin in blood) are called one of the main predictors of ASD.
ASD individuals have significantly higher 5-HTP (serotonin) levels in blood, higher kynurenine/tryptophan ratio (meaning tryptophan → serotonin pathway is working over hours):

3-5× 3-HAA, tryptophan oxidation metabolite (also radical scavenger, so it’s not THAT bad, peeps):

…And a lot more inflammatory IL-22, that plays a key role in, for example, intestinal barrier function:

Amongst that, early-life inflammation has been shown to trigger neurodevelopmental and psychiatric disorders, so that definitely stands to reason. And if we count in altered blood-brain barrier function, higher neuroinflammation will become a piece of cake. We’ll return to gut and BBB later, though!
Gut and immune system
Remember the IL-22? Me, too. Also remember IL-17a, as higher levels in mothers perpetuate the child’s autistic phenotype development.
Adding to that, autistic children have higher brain levels of the following inflammatory cytokines:
TNF (tumour necrosis factor)
interferon (IFN)
IL-1b
IL-6
IL-8
IL-12p4
The implications? Broad as hell. So, let’s focus - we have here higher intestinal permeability, higher IL-22 in blood and higher everything in the brain. Also, microbiome is altered:

⬆️ Acetate
⬆️ Propionate (can inhibit NADH formation, behaving like a neurotoxin)
⬇️ Butyrate (could potentially restore the deficiencies likely by enhancing BBB permeability)

Significantly ⬇️ SGLT1 (glucose uptake in the intestine) and ⬇️ GLUT2 (glucose transport)
⬆️ Firmicutes and ⬆️ Proteobacteria, and ⬆️ Bacteroidetes
⬆️ Clostridium
Levels of three enzymes responsible for breaking down sugars — sucrose-isomaltase, maltase-glucoamylase and lactase — ⬇️ in the ilea, or terminal small intestines, of children with autism
An impaired gut barrier can:
increase the levels of gut microbial components (e.g., lipopolysaccharide (LPS)) in the blood;
trigger the hypothalamic–pituitary–adrenal (HPA) axis;
stimulate immune responses, producing cytokines such as interferon-γ (IFN-γ), tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), and IL-4.
These immune cytokines can circulate and cross the blood–brain barrier (BBB), inducing systemic and CNS inflammation. The serum level of LPS was found to be significantly increased in ASD individuals compared to healthy controls.
Altered microbiome naturally leads to alterations in SCFA levels (aforementioned propionate, acetate, butyrate and ⬆️ valeric acid) which contribute a lot:

Sugar mhhm
Another fun thing is reactive hypoglycemia:
you have worse glucose uptake and transportation, along with lower enzymes for breaking down sugar → glucose/fructose will enter a lot later
yet insulin response is initiated via sweet taste!

The whole situation is akin to responding with full force insulin to something semi-sweetener-like:

So, not good.
Endpoints
Biopsychosocioexowheel spins, turn 1
So, let’s summarize:
Autism is multi-faceted, with important factors spanning:
parents’ genetics and epigenetics
mother’s substance use (also remember valproic acid potentially causing ASD) and inflammatory status during pregnancy + exposure to environmental factors
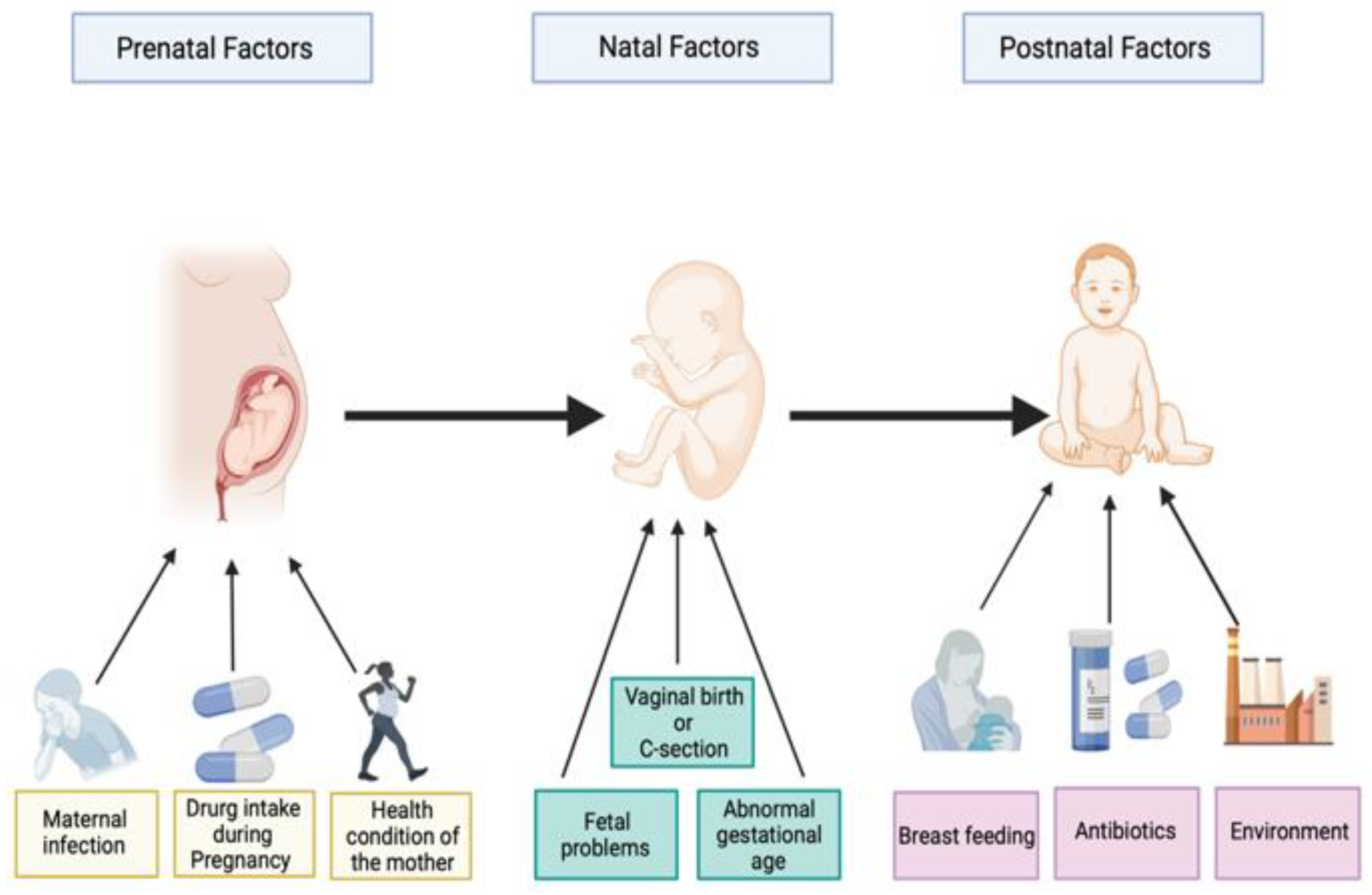
altered brain connectivity, immune status, inflammation, mitochondrial function, sugar metabolism etc.
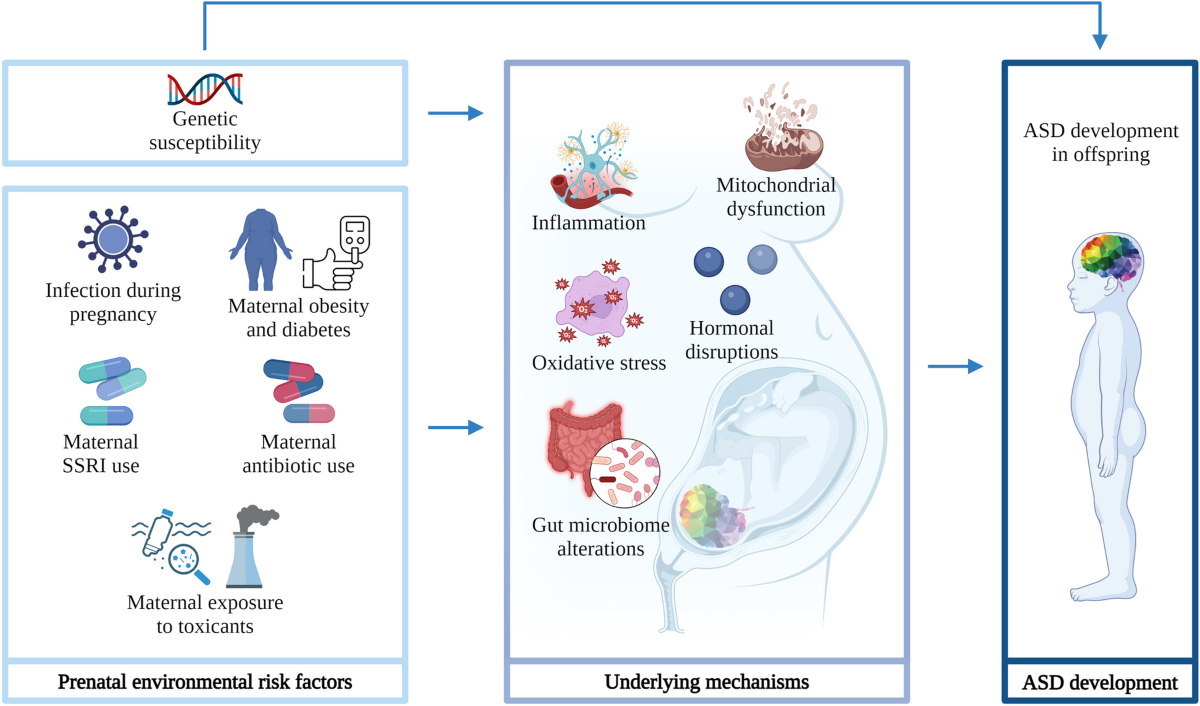
- post-natal development and early childhood can become triggers for worsening, that’s for sure
Biopsychosocioexowheel spins, turn 2
This can lead to:
altered synaptic function and density → brain regions’ development
altered BBB and gut permeability
increased inflammatory levels in gut, blood and brain
increased oxidative burden all over the body
altered sugar metabolism and energy production pathways
All this further contributes to abnormal bacterial balance in the gut → altered SCFA levels in body and brain → abnormal HDAC inhibition, mitochondrial function, inflammation, mental health etc.
Biopsychosocioexowheel spins, turn 3
Altered synaptic function potentiates the vicious cycle of motor awkwardness, social reward deficiency, being aloof → being OK with restricted interests (if you’re bullied and alone, and don’t feel like hanging out is fun - why not pursue your worlds?) → bullying/ostracism and comorbid conditions like anxiety, depression, bipolar that are just waiting to be triggered (remember pleiotropic genes?)
Another graph analysis uncovers a lot about things autistic individuals usually experience in life, and the endpoints that can lead to. It’s an unsettling image, to say the truth:
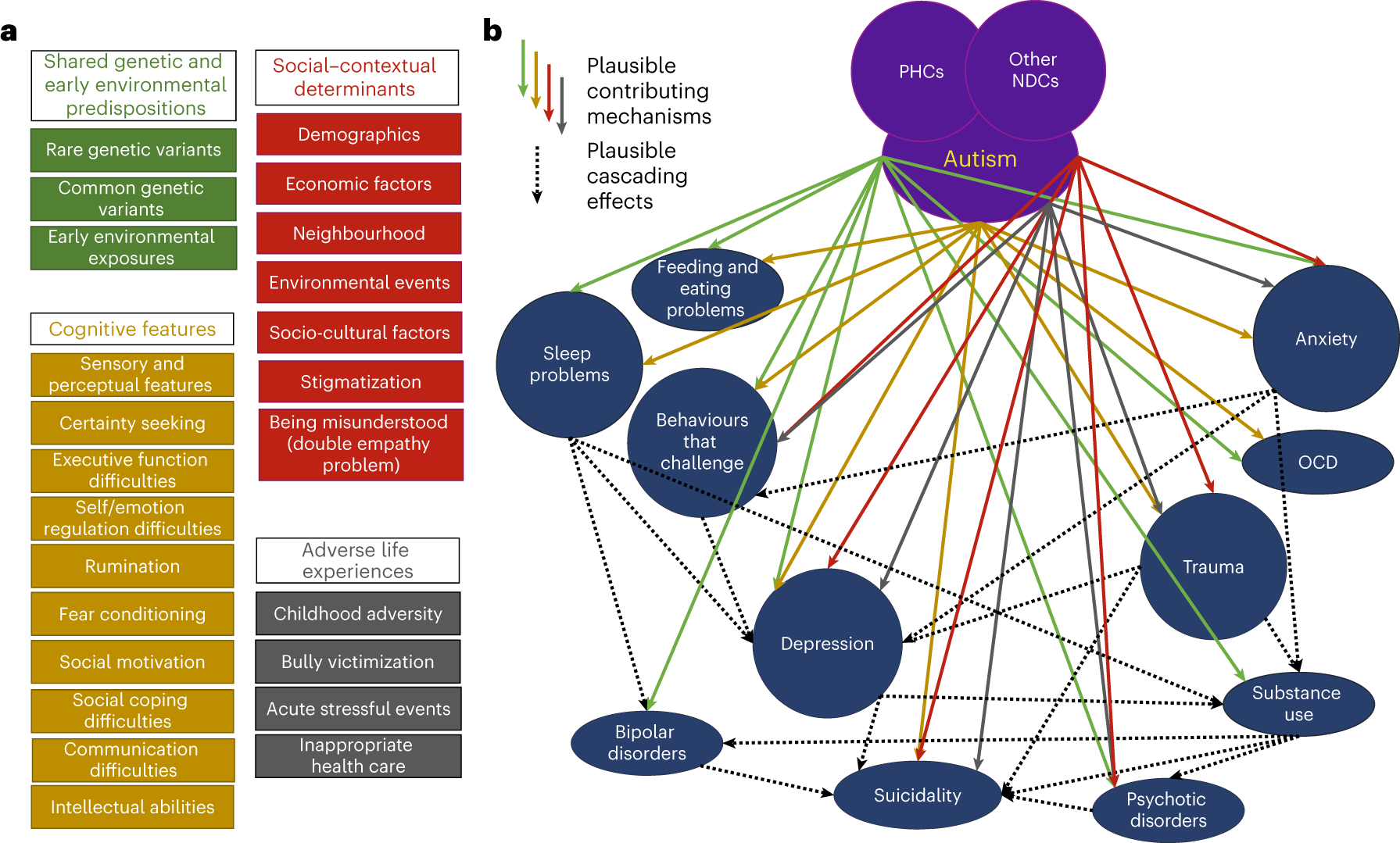
I won’t burrow into the social implications or policy changes that could IMO help (policy/incentivization will likely become the topic of some of the next posts, anyway), as that’s beyond the scope of this post.
And the final disclaimer:

Welcome to Teleogenic❣️
Other places I cross-post (not always) to: