Yet another microdosing study (full)
I just love’em.
So, after two weeks of 0.5g/day or a placebo, we’ve got almost all creativity and attention, word fluency metrics unchanged or worse:
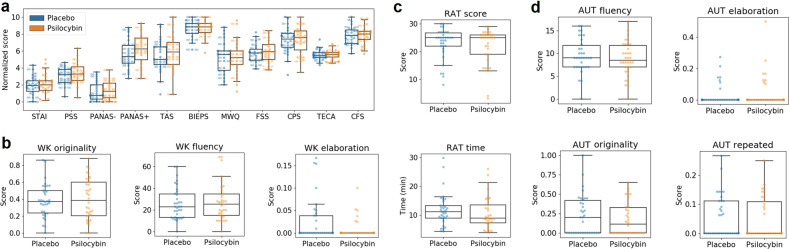
Another brick hitting the wall of measly microdosing afficionados 😌
MYT1L + mTOR ⇒ ASD/AD(H)D/etc?

There’s a rather old theory (by neuroscientific measures, IMO): less synaptic pruning → more ‘inefficient’ and synaptic circuits → autism-like phenotypes.
One of the theory facets were that upregulated mTOR led to increased connection formation which, in the absence of enough pruning, led to the aforementioned brain changes.
A recent paper had discovered another potential candidate: MYT1L, myelin transcription factor 1-like gene, may be responsible for, once again, autism-like phenotypes for essentially the same reason:
P.S. There’s even a separate syndrome called after the gene! Basically:
MYT1L helps guide brain cells to the correct parts of the brain, among other functions, e.g., controlling neuronal maturation and function + switching non-neuronal genes in neurons off
Quoting Perplexity, MYT1L also:
Controls expression of other genes associated with autism and epilepsy, including GABRB2, NR4A2, RELN, and CNR1
Regulates WNT and NOTCH signaling pathways involved in neurogenesis
Is essential for both excitatory and inhibitory neuron development
Basically, MYT1L is making sure neurons are efficient, located in the correct places and in correct quantity
We need two working copies of MYT1L; a change or deletion of one or two leads to an abundance or deficit of brain cells in different regions
Basically this can lead to a plethora of conditions, with the prime ones being ASD and epilepsy-like behaviours

Intense World Theory in its full grace
Together, mTOR and MYT1L seem to contribute to the Intense World Theory a lot:
IWT proposes that ASD (I’d add ADHD, epilepsy at least in part) is characterized by:
Hyper-reactivity and hyper-plasticity in local neural microcircuits
Enhanced perception, attention, memory, and emotional responses
This, in turn, can be caused by an interplay of dysfunctional mTOR and MYT1L, among other genes (these conditions are NOT caused by just a couple of genes - recall the Biopsychosocial model and recite it like the Bene Gesserit litany)
And the mechanism, again, quoting Perplexity:
MYT1L mutations can affect neuronal development and differentiation
Disrupted neuronal development may lead to altered mTOR signaling
Enhanced mTOR activity creates hyper-connected neural circuits
Alt therapies vs. Stimulants for ADHD

Manganese overload/burden is also presumed to play part in this, despite being crucial for SOD, the antioxidant enzyme. Excessive Mn seems to influence almost everything, mainly neurons, in an extremely negative way…
Let’s do it theses-like:
9.4% of US children have been diagnosed with ADHD
At least 23% receive no treatment
Estimated 12-68% of families (so accurate, much data) try complementary and alternative therapies to treat ADHD symptoms
~87% of pediatricians reported they had been asked about CAMs by a patient or parent in the prior three months. However, <5% reported that they felt knowledgeable about it
Some parents prefer CAMs to medications
(they don’t vaccinate, too)More patients and parents are choosing micronutrient therapy for irritability, emotional regulation, focus and attention
The fun thing is that Methylphenidate seems to, at least, not influence sleep in a bad way, likely slightly improving it!
Antidepressant discontinuation

About 14% experience AD withdrawal symptoms, with 3% experiencing severe ones (tell that to guys and gals @ SurvivingAntidepressants and get instaslamdunked)
17% of patients had symptoms that were attributable to their own expectations about stopping medications (this was accounted for in #1)
Half-life and potency are, perhaps, the main predictors of withdrawal severity, with paroxetine (extremely potent) and venlafaxine (extremely short half-life) taking the crown (tianeptine with a ~2h half-life is laughing nearby, along with clomipramine with its mega-potency)
Usual strategies suggested are: tapering incl. volumetric dosing, or switching to a longer-acting analog - there’s one king here, fluoxetine
Welcome to Teleogenic❣️
Other places I cross-post (not always) to: