Belated neuropharmacology links...
This is the COVID-I-cant-get-out-of-bed way.

Fun (?)
Google's been serving AI-generated mushroom photos 🫠
ADHD
Standard Treatment vs CAM for ADHD

CAM stands for Complementary and Alternative Medical therapies, e.g. CBT, micronutrients, not getting vaccinated…
Approximately 70% respond to stimulants and/or CBT, yet the remaining 30% just call “hey it’s a multifaceted condition, my ass”
ADHD sufferers often have decreased magnesium, zinc and iron blood levels → it stands to reason that alleviating those deficiencies can help - at least temporarily. Et voila, 54% had experienced symptom relief!
I’d still put in memantine on my short-list of “screenshot that, it’ll help” for ADH/D and ASD: IMO the “less pruning → higher excitation and excitatory propagation probability → symptoms depending on brain regions (inattentiveness, special interests, meltdowns, mysophonia, hyperfocus, you name it…)” hypothesis will hold at least partly true some day.
Surprise-surprise - methylphenidate doesn’t F up the sleep in ADHD any further, it even seems to be able to improve it slightly
ADHD algorithm
Non-stimulants (clonidine, memantine, modafinil, guanfacine etc) > atomoxetine > methylphenidate > amphetamines for the sake of safety

CBT for executive function deficits as you don’t want to prescribe adderal to anyone and everyone since childhood, pals
Own note: introduce bupropion carefully because of its seizure threshold action
Own note 2: consider lamotrigine for reasons similar to memantine (memantine may cause brain fog for some due to alpha7 nAchR blocking action)
Comorbid depression: bupropion + SSRI/SNRI
Comorbid anxiety: atomoxetine + SSRI/SNRI
The fun thing - proposed algorithm is precisely inverted:

Depression
Comorbid depression and diseases: antidepressants

Pretty much this - antidepressants can, at least partly and sometimes, decrease the risk of comorbid diseases worsening. Let’s theoritise why:
Decreasing clotting/embolism risks (less platelet serotonin → less probability of platelet activation → huh)
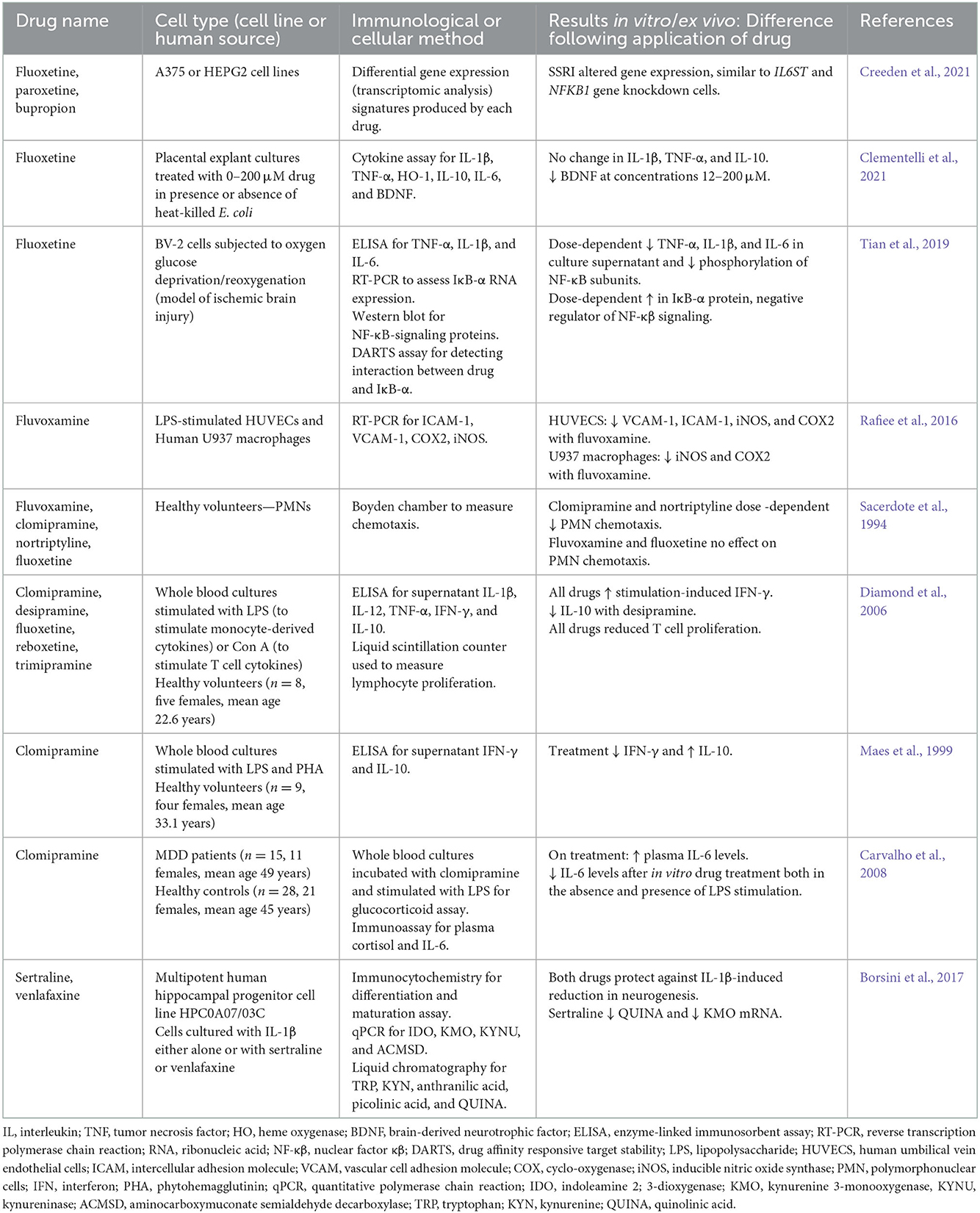
Some anti-inflammatory effects via ⬇️ TNF-a, ⬇️ IL-6:
Which Antidepressants Have the Highest Risk of Discontinuation Symptoms?

~17% of those taking antidepressants suffer from withdrawal and discontinuation symptoms (note: yeah yeah of course, just 17%)
Higher rates of symptoms emerging: imipramine, desvenlafaxine, venlafaxine and escitalopram
More severe symptoms: imipramine, desvenlafaxine, venlafaxine and paroxetine (more mechanisms + shorter half-life)
Lowest rates: sertraline and fluoxetine. Fluoxetine is often used to taper off the more ‘notorious’ medications due to its half-life. Like, after taking it for a month it’ll have inhibited P450 metabolising itself so you’ll be able to wait over for Half-Life 3
Welcome to Teleogenic❣️
Other places I cross-post (not always) to: